 Embarking in 2015, NASA astronaut Scott Kelly spent one year aboard the International Space Station while his twin brother Mark remained on Earth. Blood, saliva, urine, and stool samples were collected from both Scott and Mark during the one-year mission. While a variety of physiological markers and assessments were analyzed, two discrepancies are relevant to our interests. Firstly, a handful of Scott’s genes experienced a change in their expression during his time in space that failed to return to baseline after six months of arriving back on Earth [1]. Such an alteration is to be expected from spending a year in the stressful conditions of near-Earth space, but we will draw important implications from this finding. Secondly, the average length of Scott’s telomeres increased significantly aboard the International Space Station, an unexpected finding given that these chromosomal endcaps normally shorten with age due to a snipping that takes place with repeated cell division (though it is possible to lengthen telomeres with diet, exercise, and stress management) [2]. Upon returning to Earth, Scott’s average telomere length quickly stabilized to preflight levels.
So how do these discoveries relate to spirituality? A super quick dive into biophysics will reveal the answer. It is well known that extended exposure to a microgravity environment from spaceflight can suppress or hamper the human immune system by impacting cytoskeletons [3]. As Littleton and Ludwick suggest, cytoskeletons function as cellular gravity sensors, so microgravity exposure can muddle the regulation performed by cytoskeletons and disrupt cell motility, cell signaling, cell proliferation, and gene expression [4]. Mechanical stress or distortion stimuli are converted into chemical signals (a process termed mechanotransduction) by proteins comprising cytoskeletons and extracellular matrices [5]. Because there are physical connections between all of the tissue systems in the body, physiological changes at the organism level can be seen during spaceflight or extended exposure to microgravity [6]. Now, we know that the assembly or self-organization of microtubules (polymeric cytoskeleton components) depends on the force of gravity [7]. We also know that information can be encoded within the assembly pattern of tubulin monomers inside microtubules [8]. Furthermore, as Ostovari, Alipour, and Mehdizadeh have proposed, quantum entanglement between tubulin monomers and emitted biophotons may allow for the transmittance and exchange of both stored and accessed information throughout the body [9]. According to Sorli et al., the evolution of life is encoded within higher-dimensional Hilbert spaces and conveyed to our third dimension via biophotons [10]. Because of the quantum entanglement between microtubules and biophotons, microtubules can also partake in nonlocal interactions and transmit higher-dimensional data to the physical body through the medium of Hilbert space “pilot photons” [11]. Such data may be shuttled from biophotons to chromosomes through the vehicle of microtubule-associated proteins – allowing for a direct change to one’s DNA by way of the mind [12]. Furthering the above, physical evidence exists for gravity being able to carry with it electromagnetic data [13] [14]. And this forces us to correct the conventional definition of gravity, which is not simply one of the four forces of nature which causes apples to fall on our heads when we sit underneath trees [15]. Gravity is the toward-unity movement of consciousness units, the inward spiraling of the aether wind as the Creator wraps its arms around the universe and pulls All That Is back to it. Gravity is love, the harmonization with oneness. In other words, gravity is one half of the breath of Brahma, the inbreathing and outbreathing of the cosmos. As the planet continues onward with its ascension, additional instreams will flow from the center of the Milky Way galaxy, pass through our sun, and be delivered to the Earth. These instreams will further our consciousness elevation and greatly assist in guiding us back home. In conclusion, now we can see that we are co-creating, spiritual beings who are currently participating in a physical reality that is shaped by gravity and therefore malleable to our openness to love. The universe is perfect, but when we separate ourselves from love we perceive imperfection because we are no longer looking through the eyes of God. The completing of Earth’s evolution will entail a return to love because there is no escaping the oneness of creation. To love yourself is to love God, and to see God in all things is to see the universe as it truly is. References:
0 Comments
 Iodine is an electronegative element of the halogen family, and is an essential nutrient that must be obtained through dietary sources. Iodide is the anionic or negatively-charged form of iodine. The iodine content of foods is largely dependent upon the iodine content of the soil in which they are grown. Most foods are naturally quite low in iodine, save for most saltwater fish and various sea vegetables or seaweed [1] [2]. Undoubtedly, iodine deficiency continues to stand as a significant health issue throughout the world, affecting both industrialized and developing nations [3]. The propagandization of iodized salt is objectionable though, as conventional table salt is crap, and iodized salt can lose much of its added iodine during storage [4] [5].
Because of the need for iodine in the making of thyroid hormones, iodine is necessary for the normal development of the early brain and for general growth and maturation (in addition to the maintenance of a healthy basal metabolic rate) [6]. Iodine deficiency is one of the most common causes of preventable cognitive impairment, with a moderate-to-severe lack of iodine being associated with a reduction in mean IQ scores of 13.5 points [7] [8]. And the classical marker of iodine deficiency is enlargement of the thyroid gland or goiter [9]. Sufficient iodine intake during pregnancy is crucial, for the requirement of this nutrient rises by about 50% during the gestation period [10]. Appropriate supplementation with or adequate intake of iodine can prevent cretinism, increase birth weight, and decrease infant mortality [11]. The recommended level for iodine intake during pregnancy is at least 250 micrograms per day [12]. Ingested iodide is efficiently absorbed in the stomach and small intestine [13]. Most ingested iodine is converted into iodide in the gut before being absorbed into the bloodstream, but not all [14] [15]. So supplementing with a combination of iodide and iodine can be more effective or beneficial than supplementing with iodide (usually in the form of potassium iodide) alone. Also, selenium and iron concentrations need to be adequate in order for iodine to be properly utilized in the thyroid gland [16]. Iodide absorbed into the bloodstream quickly mixes with iodine obtained from the breakdown of iodothyronines (T3 and T4) to form the extrathyroidal pool of ‘plasma inorganic iodine,’ regulated by the thyroid and kidneys [17]. Evidently, a normal adult employs roughly 80 micrograms of iodine per day in the manufacturing of the thyroid hormones, but much more than 80 micrograms of iodine is required by the body each day [18]. For adults, the recommended daily allowance (RDA) for iodine is 150 micrograms per day, but because of our exposure to iodine-blocking pollutants, it could be argued that such a level is too low for modern needs [19]. Furthermore, we should consider that many Japanese citizens consume far more than 150 micrograms of iodine per day, and that breast cancer incidence and mortality rates have historically been much lower in Japan compared to the United States [20] [21]. A 24-hour urinary iodine test can be used to assess iodine status, but because most ingested iodine is excreted through the urine within 24 hours, results from this test can vary quite a bit [22]. Hence, iodine sufficiency is tough to measure accurately without collecting multiple urine samples [23]. And it’s worth noting that athletes or anyone who participates in vigorous exercise can lose a notable amount of iodine through sweat, so iodine supplementation could be warranted in these individuals [24]. Iodide uptake in the thyroid gland and elsewhere is accomplished via sodium-iodide symporters (membrane proteins that traffic iodide into cells), which are located mostly in the thyroid, but can also be found in the stomach, small intestine, breasts, and salivary glands [25]. Normal sodium-iodide symporter (abbreviated as NIS) function can be disturbed as a result of inflammation, a genetic defect, or exposure to environmental toxins like perchlorates and phthalates [26] [27] [28] [29] [30]. Evidence suggests that vitamin C supplementation works well for helping to repair dysfunctional sodium-iodide symporters [31]. Despite claims to the contrary, the presence of excessive iodide in the body can suppress thyroid function by inhibiting the NIS-mediated uptake of iodide in the thyroid [32] [33]. This suppression of thyroid hormone synthesis should be temporary, but there can be a failure to “escape” from the Wolff-Chaikoff effect in which the suppression is prolonged or sustained (those with autoimmune thyroiditis are more susceptible to this failure) [34]. Too much iodine can stifle autophagy in the thyroid and promote apoptosis of thyroid follicular cells as well [35]. Iodide excess can also downregulate the NIS-mediated uptake of iodide in the small intestine [36]. With all of that said, a molecular iodine dosage of 6,000 micrograms per day for five months has been administered to healthy, euthyroid women without indication of toxicity [37]. Wagner et al. observed that the maximum accumulation of iodide by the thyroid gland was achieved at a dosage of 600 micrograms per day [38]. And it has been concluded by Koutras et al. that “as the plasma inorganic iodine level rises, iodide utilization by the thyroid becomes less complete” [39]. A relatively recent estimate of total body iodine content averaged 14.6 milligrams (not to be confused with micrograms, 1 milligram equals 1,000 micrograms), the majority of iodine being concentrated in the thyroid gland [40]. Now let’s turn our attention to the known roles of iodine in the body and potential benefits that might be derived from its supplementation. Firstly, it’s important to know that bromide can weaken the impact of consumed iodide by decreasing the accumulation of iodide in the thyroid gland and increasing the excretion of iodide through the kidneys (bromine can be found in some cosmetics as well as some plastics and flame retardants) [41]. And the potency of fluoride as an antagonist to iodine is well known, with fluoride’s deleterious effects on the thyroid gland and brain being strong enough to masquerade as serious iodine deficiency [42] [43]. Chlorine and organochlorine pesticides may antagonize iodine in the body similar to fluoride too [44] [45]. Fortunately, iodine supplementation can greatly assist in the displacement and flushing out of the halides bromide and fluoride [46]. Abraham has reported that the giving of an iodide and iodine combination supplement can also promote the excretion of the toxic metals lead, mercury, cadmium, and aluminum [47]. Secondly, acute damage to the mucosa of the esophagus and stomach has been documented with the application of Lugol’s iodine, but this occurrence is uncommon [48] [49]. Placing drops of a liquid iodine solution into an enteric-coated capsule might bypass this potential issue. Moving on, iodide can serve as an antioxidant by scavenging hydroxyl radicals and defending against lipid peroxidation in cell membranes [50] [51]. The thymus gland concentrates inorganic (nonradioactive) iodine, and iodine supplementation appears to strengthen the adaptive immune system [52] [53]. Iodine can also reduce the virulence of H. pylori bacteria in the stomach as well as help normalize corticosterone secretion throughout the day [54] [55]. Stable iodine can thwart the thyroid’s uptake of radioactive iodine-131 present in nuclear fallout, but it won’t protect the body against other radionuclides like cesium-137, strontium-90, and plutonium-241 [56]. Iodine supplementation may be capable of improving the receptivity of T3 receptors, possibly via a bolstering of transmembrane iodothyronine transporters [57] [58]. Vitamin A, zinc, and fish oil may also help improve T3 receptor function [59] [60] [61]. Sufficient iodine intake might assist with the normalization of the menstrual cycle, at least in PCOS patients, in addition to possibly bettering restless legs syndrome [62]. And iodine supplementation may lower the amount of exogenous insulin needed by both type 1 and type 2 diabetics [63]. Iodine has exhibited antifungal action against the fungal species Candida albicans and antibacterial action against the bacterial species Porphyromonas gingivalis, Escherichia coli, Staphylococcus aureus, and Enterococcus faecalis [64] [65] [66]. Iodine has also shown notable antiviral activity against adenovirus, influenza A virus, Ebola virus, and HIV [67] [68] [69]. And nascent or monatomic iodine has demonstrated efficacy against Plasmodium protozoa (responsible for malaria) [70]. A low intake of iodine has been associated with a high incidence of breast cancer, and vice versa [71]. Indeed, molecular iodine has been shown to induce apoptosis in breast cancer cells, as well as outperform potassium iodide in preventing the onset of breast cancer in rats administered the carcinogen N-methyl-N-nitrosourea [72] [73]. Iodine administration has blocked breast tumor growth in rats too [74]. In a way, iodine is apparently more nourishing for the breasts, while iodide is apparently more nourishing for the thyroid [75]. A study conducted by Eskin et al. showed that abnormal mammary glands respond better to molecular iodine than they do to iodide [76]. A paper by Ghent et al. corroborated that observation, finding that molecular iodine was more beneficial for fibrocystic breast disease than iodide [77]. Iodine deficiency appears to drive the onset of fibrocystic breast disease [78]. In conclusion, there is no doubt that iodine is a critical nutrient because of its direct and indirect offices. And supplementing with iodine can surely have a positive impact on multiple physiological fronts. However, I do not agree with the recent, narrow-minded approach of administering massive amounts of iodine to the body in order to effect changes that iodine is not designed to effect. The body is an interconnected web, and when we colossally magnify one variable, we inadvertently impact the others and make it more difficult for the body to achieve and maintain a state of dynamic homeostasis. A holistic and comprehensive approach to medicine is the safe and appropriate approach to medicine. References:
 Supplemental colloidal gold exists as a sol or dispersal of gold nanoparticles in water. A colloid is simply a mixture of two substances in which the dispersed particles will not settle out. Nanoparticles are tiny, and typically have a diameter of somewhere between one and one hundred nanometers – a nanometer being one billionth of a meter. Gold colloids were first synthesized as early as the fifth century BCE and have a surprisingly long history of medicinal application [1]. For example, the therapeutic value of gold in general was supported by the Greek physician Hippocrates, the Swiss alchemist Paracelsus, and the English herbalist Nicholas Culpeper [2]. Gold is a noble metal and is normally quite unreactive or chemically inert, but gold nanoparticles can behave differently than bulk gold [3]. Gold nanoparticles scatter visible and near infrared light, so the color of gold colloids can vary [4]. In addition to the spherical geometry of gold colloid particles, various geometries in the form of nanorods, nanoshells, nanocages, and nanostars are also currently in use in the world of nanogold [5].
Gold nanoparticles have shown promise as gene therapy vehicles, being able to readily enter cells and silence particular genes by carrying small interfering RNAs to nuclei [6]. And since the uptake of gold nanoparticles by tumor cells is greater than that of normal, healthy cells, gold nanoparticles can somewhat selectively deliver anticancer agents to tumorous regions [7]. Gold nanoparticles can prevent tumors from growing by blocking angiogenesis too [8]. Impressively selective thermal ablation of diseased or infected tissue can also be accomplished with the use of gold nanoparticles because of their efficient capacity to convert absorbed light into heat [9]. Because of this ability, I personally contend that colloidal gold supplementation could extend or amplify the beneficial effects of infrared sauna therapy. Furthermore, gold nanoparticles can be conjugated with antibodies or antimicrobials and then serve as photothermal agents in selectively attacking particular bacteria and protozoa [10]. It seems that the distribution of gold nanoparticles around the body is dependent upon their size, with smaller particle sizes showing a more widespread distribution [11]. Temporary accumulation appears to be greatest in the liver, spleen, and lungs, and gold nanoparticles with a size of 50 nanometers or less may be capable of crossing the blood-brain barrier [12]. Gold nanoparticles with a diameter of less than 5.5 nanometers appear to be excreted from the body largely through the kidneys, but evidence suggests that larger particles are cleared by the mononuclear phagocyte arm of the immune system and then ultimately excreted through the gut by way of the hepatobiliary system [13] [14]. This would account for the observed accumulation of gold nanoparticles in the liver and spleen. Dykman and Khlebtsov allege that it takes about 3 to 4 months for all accumulated gold nanoparticles to be excreted from the liver and spleen, but this timescale would depend upon the size of the particles, the dosage used, and the congestion of the liver and spleen [15]. The absorption of orally administered gold nanoparticles occurs in the small intestine [16]. Gold nanoparticles with a very small size (less than 2 nanometers) can be very detrimental and can induce mitochondrial damage and tissue necrosis via oxidative stress [17]. Conflicting research exists, but the general consensus is that gold nanoparticles with a diameter of roughly 5 nanometers or greater (up to around 100 nm) in spherical colloid form are nontoxic and safe at reasonable dosages [18] [19]. And at least some reported instances of toxicity may be due not to the gold nanoparticles themselves, but to surfactants or capping agents, as well as various impurities [20]. The findings of Shukla et al. suggest that gold nanoparticles of the appropriate size are not cytotoxic and do not induce production of the proinflammatory cytokines tumor necrosis factor-alpha and interleukin-1 beta, and actually lower the making of some free radicals [21]. But again, evidence contrary to the complete safety of gold nanoparticles has been documented, so at least be wary in your purchasing of colloidal gold supplements [22]. Outside of medicine, gold nanoparticles (AuNPs) have a large range of applications in the fields of physics, chemistry, and biology, but in this article I’m going to focus on the potential benefits that may be derived from supplemental colloidal gold in its common form [23]. In a study conducted in 2007, colloidal gold administered subcutaneously inhibited the development of three forms of experimental arthritis (Mycobacterium tuberculosis-, collagen-, and pristane-induced arthritis), and the effect lasted long after treatment ceased [24]. Similar results were seen in a study where colloidal gold was injected intraarticularly into rats with collagen-induced arthritis [25]. In another study involving colloidal gold given orally to ten rheumatoid arthritis patients, nine of the patients experienced marked improvement after about five and a half months using a dosage of 30 mg/day, with three patients achieving clinical remission [26]. Interleukin-6, tumor necrosis factor-alpha, and rheumatoid factor reportedly decreased in each of the subjects. Interestingly, Abraham et al. observed a 20% increase in mean IQ scores in subjects administered colloidal gold orally for a period of one month [27]. In some of the subjects, the IQ boosting effect lasted for up to two months after discontinuation of the supplement. In a 1936 paper published in the journal Archives of Dermatology and Syphilology, the giving of colloidal gold to a single patient with lupus offered “encouraging results,” but no mechanism of action was determined [28]. Colloidal gold has also exhibited antibacterial action against the species Escherichia coli, Vibrio cholerae, Salmonella typhimurium, and Shigella dysenteriae [29]. Gold nanoparticles have also demonstrated antifungal activity against different Candida species [30]. In another interesting study, gold nanoparticles with a diameter of 21 nanometers were injected into mice through a single dose, resulting in a significant loss of fat mass without a concomitant significant decrease in total body weight (after 72 hours) [31]. The fat loss induction was apparently due to a reduction in adipose tissue macrophage activity, which we know can boost lipolysis in fat cells [32]. Something intriguing is the fact that so-called naturally-occurring gold has been found in human glandular and reproductive tissues, and in women, the concentration of this gold fluctuates with the menstrual cycle [33]. In men, Skandhan and Abraham have claimed that gold measured in normal semen is the “richest source of gold reported in biological materials” [34]. Accordingly, it has been suggested that gold may have a physiological function [35]. During the first half of the previous century, quite a few papers were published on the use of colloidal gold with arthritis patients, but that research began to taper off during the 1950s [36] [37]. At least to a degree, the “tomato effect” seems to have been operant in the medicinal employment of gold during the last few decades [38]. A wide array of claims have been made regarding the benefits of colloidal gold supplementation, but outside of the potential benefits listed in this article, to my knowledge those claims have not been empirically substantiated (and might I add that my review of the research literature was very extensive). An exception to that statement could be the Ayurvedic medicament Swarna bhasma, which when prepared correctly should contain at least some colloidal gold. Though safety concerns over impurities that can be present in the formulation have been raised [39]. In conclusion, very pure colloidal gold supplements containing no additives and made with distilled water, housing spherical nanoparticles with a diameter of more than 5 nanometers, are probably safe at reasonable dosages. Those with some form of arthritis are probably the most likely to see some kind of avail from colloidal gold’s use. But I would be very choosy in evaluating manufacturers of colloidal gold supplements as there are a lot of gold products out there that are either completely useless or downright dangerous. References:
 In order to appropriately and effectively resolve autoimmune conditions, we must understand what autoimmunity truly reflects, and the factual operation of the human immune system. Autoimmune patients cannot afford to have the mark missed in their treatment program, and practitioners cannot afford to be limited by incorrect understandings of orthodoxical, pharmaceutical-based immunology. Accordingly, let’s quickly take a look at the roles played by natural autoantibodies so that we can gain insight into the etiology of self tissue destruction.
Firstly, the immune system does not exist as simply a means for protecting the body against foreign threats, it is a body-wide conductor of our ontogeny – our growth, development, and maintenance [1]. There is an extensive yet underappreciated wisdom possessed by the human immune system, and its capacity to conduct healing of the body is immense when it is unhindered by synthetic and environmental factors. Some of that wisdom is realized and applied through what are termed natural autoantibodies. Natural autoantibodies differ from pathological autoantibodies in that their conjuring is wholly intentional and necessary, for their primary office is the averting of unwanted tissue destruction. The survival of some self-reactive immune cells and the isotype switching ability of B cells allows for the creation of natural autoantibody platoons (predominantly of the IgM and IgG classes) that regulate the body’s homeodynamics [2]. Homeodynamic stability is a more accurate concept versus homeostatic stability as it encompasses all of the complex and ongoing fluctuations from each of the body’s interwoven systems [3]. Most human natural autoantibodies are crafted by B1 cells [4]. It’s important to note that infants are much more susceptible to triggers of pathological autoimmunity because it can take over two years for significant levels of IgG natural autoantibodies to build up after birth [5]. The current CDC vaccination schedule recommends numerous vaccines before the age of two, and repeated vaccination can induce isotype switching in B1 cells that leads to the generation of confused and unchecked antibodies which target self antigens (i.e., pathological autoimmunity) [6]. Contrary to orthodoxical views, natural autoantibodies actually serve to protect against the development of pathological autoimmunity, through such means as helping to clear immune complexes, binding to microbial epitopes that resemble self epitopes, suppressing the making of proinflammatory cytokines, neutralizing pathogenic autoantibodies, and blocking the uncontrolled expansion of autoreactive clones [7] [8]. Additionally, natural autoantibodies help to clear metabolic waste from cells, remove old erythrocytes (red blood cells), thwart tumor formation, and defend against microbial infection by opsonizing or marking pathogens for elimination [9] [10] [11]. With all this in mind, we can generally view pathological autoimmunity as an overwhelming of the body’s efforts to restore equilibrium or at least mitigate disease manifestation in the face of continued tissue insults. While the conventional medicine approach to treating autoimmune disease focuses on turning off immune responses, natural medicine focuses on removing the factors responsible for tissue damage, and then assisting the immune system in doing the job it’s designed to do. This is why natural medicine is capable of correcting autoimmune disease, while conventional medicine is not. Now, unarguably the first step in remediating autoimmunity is optimizing the individual’s nutritional foundation. While honoring the individual’s metabolic, genetic, and environmental needs, beginning with the prescription of some kind of autoimmune paleo diet is often appropriate and beneficial. The short term or acute implementation of some version of an autoimmune paleo diet (does not need to be excessively or invalidly strict) can be greatly helpful for removing allergenic or immunogenic foods, correcting possible micronutrient (or macronutrient) deficiencies, and giving the epithelial lining of the small intestine a chance to reseal itself (with assistance). A whole foods-based, anti-inflammatory diet (which can be extracted from an autoimmune paleo template) can assist the body in the correction of autoimmune disease by offering an abundance of antioxidants and immune-modulating nutrients like vitamin A, vitamin D, and omega-3 fatty acids; bolstering the phase II detoxification pathway of the liver; supplying plenty of microbiota-accessible carbohydrates (MACs) or prebiotics for the reestablishment of a healthy intestinal microbiota; and facilitating the maintenance of a slightly alkaline pH within mitochondrial matrices [12] [13] [14] [15]. The use of an autoimmune paleo diet has been shown to be efficacious in a study involving fifteen subjects with inflammatory bowel disease, where 73% of the subjects achieved remission by week six [16]. Though this is not to say that autoimmune diets, whatever they may consist of, should be applied universally. Nutritional programming should always be tailored to the current and specialized needs of the individual. In conclusion, those with autoimmune disease deserve to have more than fragments of hope for the bettering of their ill-health. And with natural medicine, much more than hope can be offered. References:
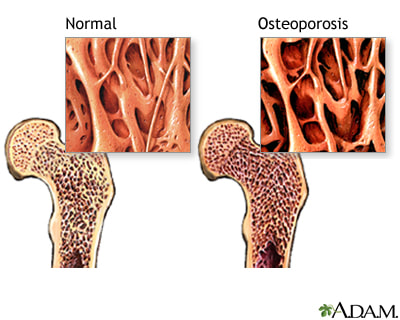 Osteoporosis is typically defined as a condition in which there is a persistent, net loss of both bone tissue and bone minerals due to an imbalance between the processes of bone formation and bone resorption. For instance, a relatively excessive blood concentration of the hormones which promote bone resorption (such as parathyroid hormone, cortisol, T3, and T4) can tip the scale toward the development of osteoporosis. Conversely, a relatively deficient blood concentration of the hormones which promote bone formation (such as HGH, IGF-1, estrogen, testosterone, calcitonin, and the active form of vitamin D) can tip the scale in the same direction. However, the etiology of osteoporosis is not unifactorial and is more complex than typically appreciated by physicians who simply prescribe hormone-replacement therapy or bisphosphonates for this condition (which is not a good idea, unless the patient is desiring to develop breast cancer, osteonecrosis of the jaw, or atrial fibrillation).
The interplay between parathyroid hormone, calcitonin, and the active form of vitamin D (1,25-dihydroxyvitamin D3) in the regulation of blood calcium levels is quite simple and well understood, so let’s focus on what is usually ignored or not well known regarding osteoporosis’ etiology. Firstly, gastrointestinal absorption of calcium is largely dependent upon a sufficient concentration of the active form of vitamin D, but “inorganic” versions of calcium (such as those found in most supplements) are very poorly absorbed and utilized regardless of vitamin D levels. Organic calcium salts (from plant-based supplements or whole foods) have been chelated or bound to a carbon-containing compound (like an amino acid or organic acid), which allows them to be more easily recognized and assimilated by the body. Conversely, the calcium present in pasteurized, homogenized milk is hardly assimilated by the human body as such milk is notably alkaline and lacks the enzymes needed for proper calcium absorption (calcium is absorbed best in an acid medium). So organically-grown vegetables (such as bok choy, cabbage, white carrots, turnip greens, mustard greens, almonds, broccoli, kale, and lima beans) are much better sources of usable calcium. Other issues which can impair the absorption of calcium include: pharmaceuticals used to treat acid reflux; surgical resection of some part of the GI tract; persistent use of glucocorticoid drugs (they promote urinary calcium excretion); and GI inflammation due to microbial infection, high sugar consumption, or gluten-related damage [1]. The second major factor that can be at play in the development of osteoporosis is the immune system’s hyperactivity due to intestinal hyperpermeability (or Leaky-gut syndrome). When business that shouldn’t be leaking out of the gut begins to, the immune system gets placed on high alert, and the adrenal glands and the liver can become notably weakened from having to respond to the onslaught of toxins/antigens. Such overactivity of the immune system can lead to an autoimmune response against osteoprotegerin (a glycoprotein which inhibits bone resorption), which can contribute to osteoporosis by increasing the rate at which bone is resorbed [2]. The toxins leaking out of the gut can also damage the hormone receptors embedded within the membranes of bone cells, so that the hormones which promote bone formation become less effective at doing so. The last factor we’ll discuss is strongly tied to the first two. To avoid going unnecessarily deep, the liver uses alkalizing minerals (such as calcium and sodium) to assist in its detoxification duties. When the liver is forced to deal with an onslaught of acidic toxins (from a leaky gut), it can begin protecting its sodium reserves, forcing the body to begin pulling calcium from the bones to buffer the acidic toxins [3]. Furthermore, an overly-taxed liver will be less efficient at recycling estrogen, which can forestall estrogen’s beneficial influence on bone formation (especially in women). A stressed liver can also pass on un-detoxed toxins to the kidneys, which can interfere with calcium reabsorption by the kidneys. Lastly, a leaky gut (and any excessive or persistent stress in general) can overstimulate the adrenal glands and their release of cortisol, which decreases intestinal absorption of calcium – this indirectly leads to a secretion of parathyroid hormone (which increases osteoclast or bone-resorbing activity). So you can see that simply prescribing estrogen, a calcium/vitamin D supplement, or bisphosphonates does not effectively correct the underlying progenitors in the development of osteoporosis. Of course, depending upon an individual’s specific etiology, a different resolution plan may need to be instituted, but I hope this article was helpful in illuminating the true origins of osteoporosis as conventional medicine’s typical understanding of this condition is embarrassing. References:
 While the development of Type 1 diabetes (T1D) in humans is obviously multifactorial, the formation of recent understandings regarding intestinal hyperpermeability (“Leaky-gut syndrome”) and autoimmunity has shed significant light on a major progenitor in the development of T1D. Traditionally, the etiology of autoimmune conditions was largely limited to the events of molecular mimicry (foreign invaders resembling non-foreign components of the body), the bystander effect (abnormal activation of autoreactive T-cells by microbes or xenobiotics like heavy metals), and viral persistence (activation of antiviral immune responses to previously dormant viral antigens) [1] [2]. While the mechanisms associated with molecular mimicry, the bystander effect, and viral persistence have certainly been shown to elicit autoimmune responses, the development of intestinal hyperpermeability may strongly outweigh the typically identified progenitors for the manifestation of autoimmunity – T1D in particular.
The permeability of the intestinal lining is largely regulated by the protein zonulin, which through a cascade of receptor activation, elicits the disengagement of the protein complexes forming the tight junctions between epithelial cells lining the intestinal wall [3]. The zonulin pathway normally functions in modulating the selective transfer of fluids, macromolecules (such as digested food particles), and leukocytes (immune cells) between the blood circulation and the intestinal lumen (the small intestine interior) [4]. Additionally, the zonulin pathway within the GI tract is also believed to play a role in protecting against the colonization of unwanted microbes within the small intestine (however, SIBO can excessively induce the production of zonulin and procure the development of Leaky-gut) [5]. I’ve written an article on SIBO if you want to know more about that. One of the most potent upregulators in the production of zonulin is the gluten family of proteins, gliadin being the chief troublemaker. Gliadin binds to a particular receptor embedded within the intestinal lining and elicits the release of zonulin and the subsequent increase in intestinal permeability [6] [7]. This upregulation invoked by gliadin takes place in all human beings, not just those with Celiac Disease or Non-Celiac Gluten Sensitivity [8]. For those with T1D, it should be noted that a similar immunological response to the ingestion of gluten can be invoked by the ingestion of A1 beta-casein protein from dairy products stemming from A1 cows [9] [10]. Accordingly, the removal of gluten and A1 dairy sources from the diet can be a requisite for the resolution of autoimmune conditions, especially for those who are knowingly or unknowingly gluten sensitive [11] [12]. Along similar lines, a direct link has been mapped between a specific protein found in wheat (Glo-3a), the upregulation of zonulin, and the attacking of pancreatic beta cells in those exhibiting a genetic susceptibility to the onset of T1D [13]. This pancreatic autoimmunity can be exacerbated in those who have a degraded mucosal barrier within the small intestine, which can be brought about by inflammatory action within the gut (the same inflammation can also increase the gut’s permeability in and of itself). Multiple experiments have demonstrated the onset of T1D being preceded by an increase in intestinal permeability, and the GALT (gut-associated lymphoid tissue) easily plays one of the chief roles here [14]. The transportation of lymphocytes (immune cells) from the GALT to the pancreas is mediated by a particular molecule (MAdCAM-1) and a particular integrin (alpha 4 beta 7) whose expression is elevated in those with T1D [15]. Thus, one mechanism through which T1D may manifest in an individual is as follows: a foreign antigen (or antigens) from within the GI tract, whose delivery to the pancreas is facilitated by intestinal hyperpermeability (Leaky-gut) stemming from zonulin upregulation by such provokers as gluten, beta-casomorphin-7 (from A1 cow’s milk), heavy metals, or certain microbes, promotes the onset of pancreatic autoimmunity in a genetically susceptible person [16]. Therefore, in reversing the above etiology, the gut lining would need to be healed, the gut microbiota would need to be restored to normal, and the foreign antigens present within the blood/lymphatic circulation and extracellular matrices would need to be detoxified and excreted from the body. While the reversal of autoimmune conditions certainly can and has been done, it is important to remember that each individual’s etiology may be unique, and thus may require a very individualized program to bring the mind and body into a state of equilibrium, in which natural functionality and health may be expressed by default. References:
 I’ve discussed the primary progenitor in the development of autoimmunity as being intestinal hyperpermeability (or Leaky-gut) in many previous articles, so here I would like to cover some other players that are strongly involved in the processes of autoimmunity, as well as in the natural expression of health in general. As a quick refresher, because of the strong ties existing within the gut-brain axis, inflammation present within the GI tract can lead to hyperactivity of the immune system and a leaky gut can flood the body with toxic material that perpetuates immune-hyperactivity and cellular inflammation.
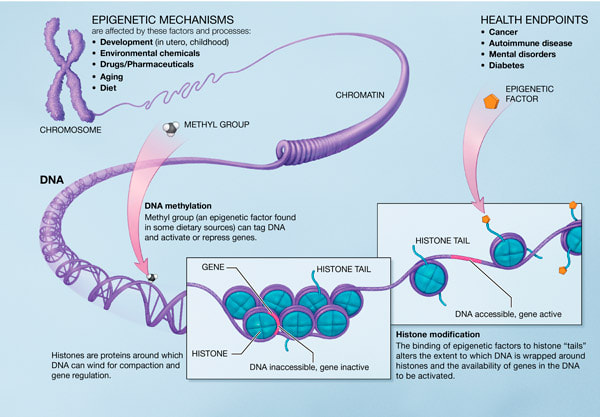
Exposure to genetically-modified foods, herbicides and other pesticides, heavy metals, pharmaceuticals, discordant electromagnetic radiation, artificial preservatives, and industrial pollutants can all alter the fashion in which facets of our genetic blueprint are expressed. Contrary to the “Central Dogma” B.S. that still pervades conventional medicine, our first layer of DNA (the aggregate double-helix) largely serves as a blueprint and factory, but the foreman reading the blueprint and directing construction is the collective environment (including our thoughts, beliefs, and emotions). Thus, one’s genetic blueprint is not a “health fabric” that simply unfolds in a predestined manner, it is a toolkit that the body’s consciousness uses to build the body’s composition and adapt to an ever-changing environment. So it is our environment that determines how our genetic blueprint is expressed, which quite simply provides the biochemical and biophysical basis through which you have broad dictation over the health of your physical body. Along similar lines, the human genome was patterned after the natural elements constituting this planet, and what the human organism would normally be confronted with in the environment. This is one of the main reasons why the body is designed to respond to and cooperate with naturally-occurring substances, not synthetic creations (such as pharmaceuticals) which obstruct information pathways and hinder the mechanisms used by the body to heal and sustain itself. It is organic foods and herbs that provide beneficial, epigenetic instruction and influence to the body. It is organic foods and herbs that assist histones in the correct folding of DNA helices so that appropriate operations may be expressed. And it is organic foods and herbs that assist in the repairing of chromosomal damage invoked by the plethora of toxins we are now exposed to on a daily basis. Now, without delving too deep, much of the biochemical, healing assistance facilitated by organic foods and herbs is mediated in part by methylation processes. Methyl groups might be viewed as pervasive switches which play a huge role in regulating a large number of cellular activities by adding themselves or removing themselves from RNA, DNA, proteins, toxins, and other molecules [1]. A deficiency of methyl donors (due to a lack of dietary folate, choline, betaine, vitamin B6, vitamin B12, or depletion from oxidative stress) can give rise to a large number of issues, but perhaps of chief interest is the fact that one can become locked into a persistent activation of the stress response [2] [3]. This locking into activation of the stress response not only steals needed methyl groups from other bodily processes, but also perpetuates cellular inflammation and can facilitate the development of autoimmunity through invocation of the “no/onoo” cycle (a vicious cycle of elevations in nitric oxide and peroxynitrite) [4]. Sustainment of the no/onoo cycle can also lead to chronic fatigue syndrome, multiple chemical sensitivity, fibromyalgia, heart failure, and a host of other inflammatory diseases. Accordingly, because there are few diseases or conditions of ill-health which do not stem from chronic inflammation or chronic activation of the stress response, ensuring the body maintains an adequate supply of methyl donors can be extremely important in the correcting of physiological imbalances and the healing of disease states. References:
 In this short post I thought I’d quickly go over a few things that are often ignored or unknown in the development of “fat-loss resistance” (and excess adiposity) so that you can be better equipped to correct such a condition. As I’ve already discussed in other articles, weight gain and weight loss are by no means a simple energy balance issue. An enormous matrix exists for the regulation and improvement of one’s health (both physically and non-physically) and therefore the pattern in which adipose tissue is deposited or removed. Today let’s focus on the state of one’s gastrointestinal tract and the health of one’s microbiome (the collection of genomes from all of the microbes inhabiting the body).
Everyone develops a microbiome that is unique and specific to them as the collection and proportion of microbes that end up inhabiting one’s body are genetically- and environmentally-determined (the environment being the much larger determinant). Some of the most important factors which help to shape one’s microbiome early on include: gestational age, vaginal vs. C-section delivery, having been breast-fed vs. formula-fed, antibiotic use, infant hospitalization length, and of course the health and diversity of the mother’s microbiota. Looking at two dietary factors that can disrupt the microbiome, a low intake of prebiotics or fiber as well as an excessive intake of lipids for your metabolic type can promote the proliferation of pathogenic, gram-negative bacteria, which can then increase your exposure to lipopolysaccharides (also known as endotoxins) as bad bacteria house these endotoxins in their cell walls [1]. An increase in lipopolysaccharide (LPS) concentration is bad news for fat loss for two primary reasons. The first of which is the decrease in one’s protection against organochlorines (often used in pesticides) that can invoke estrogen dominance (promoting fat gain) and a lowering of active T3 levels (decreasing one’s metabolic rate) [2]. The second reason is the manner in which LPSs facilitate inflammation in the gut, Leaky-gut development, and the onset of an inflammatory cascade once they breach the gut lining [3]. The initiation of this inflammatory cascade can encourage the development of insulin resistance, a release of pro-inflammatory cytokines from adipose tissue, a lowering of thyroid hormone output, and a blocking of thyroid hormone receptors (all of which strongly nullify attempts at fat loss) [4]. Furthermore, an increase of LPS entering the bloodstream can promote a notable shift toward gluconeogenesis (new glucose formation) which can pull glutamine and other amino acids out of the gut lining, further exacerbating the leaky gut and inflammatory cycles. Under this condition, amino acids can also be pulled from muscle tissue, degrading your major metabolic furnaces and decreasing your ability to oxidize fat tissue. So what are some things you can do to improve your gut health? This depends on the person and whether or not they have any microbial infections, a leaky gut, low stomach acid, poor pancreas function, a stressed liver, and other considerations but here are some general recommendations:
References:
 While there exist multiple techniques for or approaches to stretching the body, I feel it is safe to say that the static stretching of muscles (or similar connective tissues) is the modality most often employed. There are a few things I would like to quickly state regarding static stretching in order to hopefully highlight why it is that this technique is often fruitless as the arena of stretching can be a little confusing (even for those with a strong background in this stuff).
The first item of business revolves around the fact that it is the nervous system which dictates the length and tone of muscles, so it is the nervous system which must be addressed when attempting to restore a muscle’s length and/or tone. Simply employing traditional, static stretches for short, tight muscles without correcting the reason(s) why those muscles are short and tight will usually be pretty futile. To be more precise, every skeletal muscle fiber’s length and tone is determined largely by one’s sensory-motor system (specifically the alpha-gamma feedback loop). Covering the details of this determination is unnecessary here but during the learning of a particular motor (or movement) pattern, when an equilibrium is reached between the input stemming from what are known as ‘alpha and gamma motoneurons’ (which are responsible for innervating extrafusal and intrafusal fibers, respectively), an assumed appropriate length and tone for the corresponding muscle fibers will be established. Therefore, in order to alter any established length or tone of a muscle it is this neural pattern which must be reset. This resetting can be effectively accomplished with the use of Somatic exercises which I cover in a couple of my e-books if you care to learn more. So only considering the effect of mechanically stretching any type of connective tissue (muscular, tendinous, ligamentous, skeletal, or fascial) regrettably ignores the fact that the length, tone, and response to stretch of any connective tissue is only partly dictated by the state of the tissue structure itself (such as the number of collagen fibrils present, the degree of elongation or deformation of those fibrils, the pattern of remodeling present and active within the tissue, etc.). To say things differently, having a normal range of motion at each joint is innate for the human body (with some rare exceptions), so normal muscle flexibility is only lost when a program is implanted in the nervous system which alters the nervous system’s maintenance of an appropriate length, tone, and extensibility of a muscle. Of course, multiple forms of stress and usage patterning can induce changes in the architecture and composition of connective tissues which could limit the normal extensibility of a muscle, but I’m mainly trying to explain that the simple static stretching of a muscle in order to maintain one’s flexibility or to correct a flexibility issue is rarely going to elicit the results desired. Some of the forms of stress or dysfunctional programming that can inhibit one’s natural flexibility include: improper neuromotor conditioning (learning or practicing how to use or move the body incorrectly), dysfunctional postural carriage (such as forward head posture or rounded shoulders), inadequate nutrition (such as pro-inflammatory diets which easily force postural and movement compensations through what are termed “viscero-somatic reflexes”), restraining psychological and/or emotional patterns held within either the fascial matrix or one’s auric field (which often stem from avoiding or suppressing “negative” thoughts or emotions), hormonal imbalances (such as those stemming from blood sugar levels fluctuating excessively), toxin exposure/accumulation (toxins often settle in extracellular matrices and prevent normal exchange of nutrients and waste as well as inhibit normal movement of tissues), adhesions from muscle spasms or scar tissue formation (which can not only perpetuate inflammatory business but can also alter recruitment patterns and postural carriage), and even imbalances or obstructions within the chakra systems or meridians. So you can see that there are multiple factors which can be at play in the condition of muscles remaining in a short and tight state. With all of this in mind, a more appropriate objective for restoring flexibility would be the returning of the individual or oneself to a state of holistic health, because when that state is achieved one’s normal joint ranges of motion can return without the need for attempts at forcing muscles to lengthen (which can be counterproductive). With that said, simply using some basic self-myofascial release techniques or receiving a good ol’ fashioned massage can be significantly helpful in correcting modest problems that often inhibit normal flexibility from being expressed. Have a good week!  In this short article let’s talk about soft tissue inflammation arising from mechanical injury and why the use of ice (or cryotherapy in general) impairs the body’s natural healing response. To begin, let me provide some background on the “swelling” process. Because of the negative electrical charge carried by many macromolecules and proteins within the cytoplasm of most cells (here I’m focusing on muscular, ligamentous, tendinous, and fascial tissue), an osmotic draw is present within most cells, in which extracellular water is attracted to the cell interior. However, cellular cytoskeletons and macromolecule networks provide a rigidity to cell structures that prevents an unabated influx of water into cells, so intracellular water levels normally remain relatively low (emphasis on relatively, cellular hydration is extremely important) [1].
When there is mechanical injury to soft connective tissue (such as muscular or ligamentous tissue), the same cytoskeletons and macromolecule networks that normally prevent excessive osmotic draw can be damaged or disrupted, allowing fluid to progressively but quickly flood the tissue. This is the primary mechanism by which soft tissues swell after mechanical injury (there’s also an increase in cell membrane permeability). So in order for excess fluid to be removed from the interior of cells and to prevent excess fluid from continuing to enter cells, the cytoskeleton and molecular networks need to be repaired and restored to their usual organization. However, the swelling action is highly regulated and is a critical step in the three-phase healing response. The first of these three phases is the acute inflammatory phase, in which the injured area is quarantined off and stabilized. The repair phase follows, in which the primary activity consists of fibroblasts repairing connective fibers and matrices. Lastly, the remodeling phase finalizes the healing response through the shaping and orienting of tissue structures in a manner that is in line with the patterns of stress experienced by the tissue undergoing healing. Under normal circumstances, the entire healing response is an autoregulated and self-limiting one, which means that Mother Nature never intended for us to mess with it. When we do mess with it, through the use of ice or NSAIDs (nonsteroidal anti-inflammatory drugs such as Ibuprofen), we interfere with the prostaglandin- and cytokine-mediated inflammatory response (which is necessary!) which corrupts the repair and remodeling phases [2] [3] [4]. Icing injured soft tissue increases the permeability of surrounding lymphatic vessels which creates a backflow of lymph into the interstitial space (lymphatic vessels operate as a one-directional highway fueled by the negative pressure created mostly by muscular contraction). This backflow worsens congestion around the injured site, obstructing the main avenue through which cellular debris and waste products from the damaged tissue escape (through the lymph), and impairs prostaglandin release [5]. The impairment of prostaglandin release can forestall the direction of macrophages to the injured site (inhibiting the normal cleanup of cellular debris) and forestall the action of IGF-1 (insulin-like growth factor 1, chaperoned by the macrophages), impeding cellular healing. In other words, the use of cryotherapy techniques muddles the healing process from completing correctly, perpetuating the inflammation, swelling, and pain that cryotherapy employment seeks to mitigate! Accordingly, instead of adhering to the bogus RICE principle (which every textbook relating to sports medicine still propagates), after a soft tissue injury one should apply gentle heat to the injured site as well as actively contract the musculature at or near the injured site. This approach facilitates the delivery of requisite nutrients to the damaged tissue, the removal of waste material through the lymphatic system, and the proper organizing of connective components constructed during phase three of the healing response. So if your physical therapist, orthopedist, or sports medicine professional tells you to ice your next ankle sprain, congratulations! It’s now time to find a new physical therapist, orthopedist, or sports medicine professional. Have a great day. References:
|
AuthorDenton Coleman is an Exercise Physiologist and Medical Researcher. Archives
October 2023
Categories |

 RSS Feed
RSS Feed
